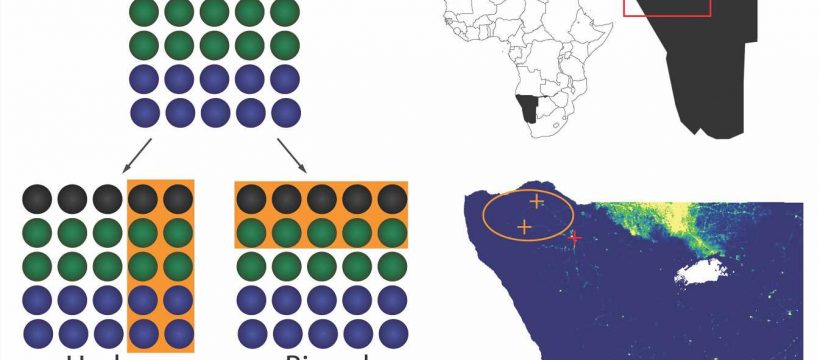
 Schematic showing underrepresentation and biased representation of a population. Circles represent individuals; black, blue, and green colors each represent one of three possible values for a demographic characteristic. Orange shaded areas represent individuals selected for inclusion in each data set. (B) Above: Inset map of continent, Namibia in black, and region of interest outlined in red. Below: Detailed map of the region of interest showing population density in 2016 (yellow = high; blue = low; white = NA (Etosha National Park, no human population)). Study area circled in orange, health clinics (orange crosses), regional hospital (red cross). Map created in ArcGIS with data from GADM (https://gadm.org/). Credit: PLOS Digital Health (2023). DOI: 10.1371/journal.pdig.0000270")
Mobile phone data are increasingly used in public health management and disease outbreak response, as demonstrated during the COVID-19 pandemic when location data were used as a proxy for human movement and contacts and informed exposure notification apps. However, a new study led by researchers at Penn State revealed that phone data may not accurately reflect under-resourced or particularly vulnerable populations, who are often underrepresented in other data as well.
If this bias is not acknowledged or complemented with additional data, the researchers said, a reliance on phone data in public health efforts could magnify health inequities. They published their findings today (July 6) in PLOS Digital Health.
“Populations with limited access to health care are also often overlooked in other data sources, including censuses,” said Nita Bharti, associate professor of biology in the Penn State Eberly College of Science and leader of the research team. “New, convenient data sources like mobile phones can offer important insights into these populations, but it is critical that we identify and measure their biases.”
Data gaps exist in all contexts and can be easily seen in small, rural populations, according to Bharti. In this study, the researchers investigated phone ownership, mobility and access to health care in a mobile, rural population in Namibia as a case study to measure mobile phone data representativeness in populations that regularly experience vaccine-preventable infectious diseases.
Namibia is a middle-income country in southern Africa, and Bharti said mobile phone data from the region are used to guide public health decisions around malaria and other infectious diseases. Most Namibians live in urban areas with reliable access to health care, but this is not the case for rural or remote populations. The research team conducted detailed surveys of more than 250 people at two settlements in a remote area of the Kunene province. Residents are largely nomadic, moving seasonally to herd cattle, and the distance to the nearest health clinic is substantial.

The researchers found that phone ownership was relatively low, with only 31% of participants owning a phone—compared to the estimated 95% in urban areas in the country in 2013—and only 59% having used a phone in their lifetime. Phone owners and users were far more likely to be men, to travel to more locations and to have better access to health care.
“We found that, within these already vulnerable populations, the most vulnerable people were underrepresented in these phone data because they didn’t own phones or have access to phones,” said Alexandre Blake, graduate student in Bharti’s lab at Penn State and first author of the paper.
“One common way to make up for missing data is to simply scale it up and assume that missing data are the same as recorded data. But we distinctly found that the people missing in phone data are less mobile with reduced access to health care. And with respect to making public health decisions, these are very important differences.”
Mobile phones also provided a skewed perception of mobility among phone owners, according to Blake. Because phone owners frequently traveled to areas with no phone reception, many of their movements would not be captured in phone data.
“Even if you own a phone, you can only be tracked in locations where you get signal,” Blake said. “So, phone data, especially from remote areas, will only capture a specific segment of the population and can record only some of their movements. If phone data were used to predict the potential spread of an infectious disease in a region like the one we studied, most movements and contacts would be missed. Without accounting for data biases, movements based on phone data would be misleading and ineffective for outbreak response efforts attempting to limit the spatial spread of a disease.”
Because mobile phone data may not accurately represent the populations and locations that most need public health improvements, the researchers suggested that relying on these data to inform public health decisions can actually be harmful and potentially magnify health inequalities. They stressed the importance of acknowledging and measuring bias in all types of data—not only those used for public health—as well as using multiple types of data with non-overlapping biases when drawing conclusions.
“All data have biases but are still valuable resources, and phone data are no exception,” Bharti said. “Acknowledging that data are not just under representative and showing that they are in fact biased helps our field move towards correctly interpreting data, measuring biases and looking for ways to measure what’s missing.”
According to the researchers, small, remote populations play an important but often overlooked role in the transmission and persistence of infectious disease. Limited access to health care can lead to delayed detection of outbreaks, and overlooking these groups can slow the elimination of vaccine-preventable transmissible pathogens.
“Equitable access to health care is a basic human right, and addressing health inequities in underrepresented populations is essential for public health progress,” Bharti said.
“You don’t have to look to low- or middle-income nations to find underrepresentation in vulnerable groups. We would see the same absence of vulnerable groups in widely used data if we looked, for example, at a rural part of Pennsylvania or Mississippi or in urban areas, like New York City or Los Angeles. There are gaps and biases in all data that underrepresent the segments of populations most in need of improved health services. Failing to acknowledge these biases can direct resources away from these groups and lead to public health interventions that magnify inequities.”
In addition to Bharti and Blake, the research team includes Ashley Hazel at the University of California, San Francisco, and John Jakurama and Justy Matundu at the Kaoko Information Center in Namibia.
More information:
Alexandre Blake et al, Disparities in mobile phone ownership reflect inequities in access to healthcare, PLOS Digital Health (2023). DOI: 10.1371/journal.pdig.0000270
Journal information:
PLOS Digital Health
Source: Read Full Article