
Cardiac conditions in women are underdiagnosed, undertreated, and under-researched compared to those in men. In a prospective study in the Canadian Journal of Cardiology, investigators report that attending a multidisciplinary dedicated women’s heart center can increase the likelihood of an accurate diagnosis and significantly improve clinical and psychological outcomes of women reporting chest pain due to insufficient heart-muscle blood flow (myocardial ischemia) but not diagnosed with obstructive coronary artery disease.
Cardiovascular disease (CVD) continues to be a leading cause of hospitalization and death in women. Declines in CVD death rates have stalled in mid-life women compared to men, suggesting sex-specific approaches may be needed.
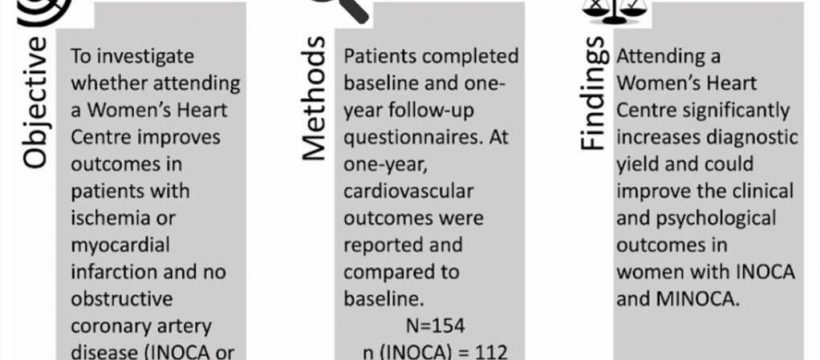
Many women with cardiac chest pain and ischemia or myocardial infarction do not have significant blockages in the arteries supplying the heart (obstructive coronary artery disease). Ischemia with no obstructive coronary artery disease (INOCA) may affect up to 62% of women undergoing coronary angiography for suspected angina, with a higher prevalence in mid-life women aged 45-65 years. Myocardial infarction with no obstructive coronary artery disease (MINOCA) accounts for 6% of myocardial infarctions and is more frequently diagnosed in women. Studies suggest that patients with INOCA and MINOCA have a decreased quality of life and are at increased risk of cardiovascular events like heart attacks and acute heart failure.
“Most studies of heart health consist primarily of male participants, and numerous clinical outcomes such as patient symptoms and treatments do not therefore necessarily apply to women with certain types of heart disease,” explained lead investigator Tara L. Sedlak, MD, Vancouver General Hospital Department of Cardiology, University of British Columbia Faculty of Medicine, and British Columbia Women’s Hospital, Vancouver, BC, Canada. “We conducted this research to gain a better understanding of the etiologies and treatment of women with ongoing signs and symptoms of INOCA, which is one of these understudied areas in heart health.”
Investigators prospectively followed 154 patients (112 INOCA and 42 MINOCA patients). attending the women’s heart center at Vancouver General Hospital, who completed baseline demographics questionnaires. Median age was 59, and the most common referral was for chest pain (94% in INOCA and 66% in MINOCA). After one year, chest pain frequency, quality of life, depression/anxiety symptoms, and cardiovascular outcomes were compared to baseline.
Many women with cardiac chest pain and ischemia or heart attack have no significant blockages of their larger coronary arteries but can have narrowing or dysfunction of their small coronary vessels or spasm of their blood vessels, which may be missed at initial diagnosis.
At baseline, 64% of INOCA and 43% of MINOCA patients did not have a specific diagnosis. Following investigations in the center, 71% of INOCA patients established a new or a changed diagnosis (the most common of which was coronary microvascular dysfunction at 68%), while 60% of MINOCA patients established a new or change in diagnosis (the most common of which was coronary vasospasm at 60%). At one year, participants had significantly decreased chest pain, improved quality of life and improved mental health.
“To our knowledge, this is the first prospective report of the outcomes in Canadian women with chest pain who have attended a women’s heart center,” noted Dr. Sedlak. “We hope our findings highlight the importance of having a dedicated women-specific heart center, which provides comprehensive care for women with heart disease by providing risk factor assessment, referral to psychiatrists, exercise classes, smoking cessation treatment, and consultation with a dietitian in addition to a focus on conditions such as INOCA that are more common in women.”
In an accompanying editorial, C. Noel Bairey Merz, MD, Barbra Streisand Women’s Heart Center in the Smidt Heart Institute at Cedars-Sinai, Los Angeles, CA, U.S.. and colleagues congratulate Dr. Sedlak and coinvestigators on this important study as one of the first in Canada to showcase the improvement in outcomes for women with INOCA or MINOCA through a specialized women’s health center.
Source: Read Full Article