

Marlin Mowery was in Texas, participating in a new employee health and wellness program for his company, when he had a heart attack. It was his first meeting of a two-day workshop, and he had done one of the program’s morning workouts an hour earlier. “At 9:05, I broke into a tremendous sweat,” he recalls. “There was water literally running off my fingers.”
Although the Burlington, New Jersey, operations manager was slightly overweight, out of shape, taking medication for high blood pressure, and eating meals on the go, he figured he was just extremely fatigued. After all, he was only 50. It couldn’t be a heart attack.
So he powered through the rest of the day despite persistent sweating, nausea, and then pain in his back and ribs at night. By morning he felt so weak he could barely lift his laptop, and he finally headed to an urgent-care clinic. When an EKG discovered a massive heart attack in progress, an ambulance rushed him to a hospital, where doctors cleared a blockage in one of his coronary arteries. “You should be dead right now,” an amazed cardiologist said. Only in recovery did Mowery learn exactly what had happened. He’d just survived the mother of all heart attacks: the widowmaker.
What Is the Widowmaker?
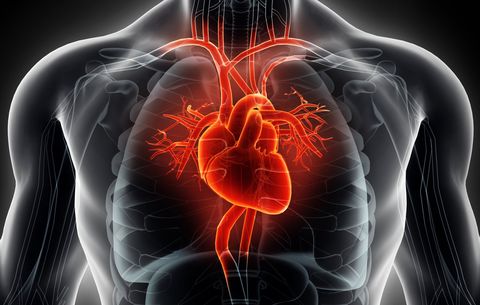
Any heart attack can be fatal, so the widowmaker isn’t unique in that respect. What makes it notable (and feared) is where it occurs: in the left anterior descending artery. The LAD provides blood and oxygen to the entire front of the heart—a larger area than other coronary arteries supply. A clog in the LAD cuts off about 40 percent of the heart’s blood. No other blockage in any other artery affects that much acreage.
“It’s a larger heart attack with higher risk of resulting complications,” says Steven Bailey, M.D., chief of cardiology at the University of Texas at San Antonio. Those complications include irregular heartbeat, heart failure, and (less frequently) sudden death.
“Sudden” can mean minutes once complications such as arrhythmia kick in, or a heart attack can span hours, as was the case with Mowery. There’s a widely varying window of opportunity to stop the heart attack before it kills. But “a third of sudden cardiac deaths in the U.S. are widowmakers,” Dr. Bailey notes.

Brian Stauffer
Besides being lethal, the widowmaker has the horror-villain trait of stealth. Half of the men who die suddenly of coronary heart disease have no prior symptoms. Many are seemingly healthy and fit. Between the ages of 30 and 60, men account for about four times as many coronary-heart-disease deaths as women. (Researchers speculate that estrogen may offer some protection that is lost after menopause.) That helps explain why heart disease kills more men in the United States than any other cause—accounting for about one in every three deaths.
There is one consolation: A clogged artery can now be quickly cleared with timely treatment. In most cities, you’re 30 minutes from a heart center with a catheterization lab. (If you’re farther away, EMTs can keep your ticker ticking with drugs until you get there.) Then a cath lab’s interventional cardiologist can perform an angioplasty—threading a thin tube (catheter) into the blocked coronary artery and expanding it by inflating a small balloon. Most people undergoing angioplasty will also have a stent installed to help keep the blood vessel open.
“It’s like there’s a dead end at the end of a road, and that’s where the blockage is,” says Mowery, who watched his angioplasty live on a screen. “Once the road is open, your whole body relaxes.”
Whether you survive depends on severity, complications, and, yes, luck. “If you’re seen within the first two hours, survival can be as high as 96 percent specifically as a result of what the interventional cardiologist does,” explains Dr. Bailey. So the widowmaker doesn’t have to make actual widows.
But such advanced and available treatment still won’t prevent approximately 421,000 men from dying of cardiovascular disease every year. It’s up to you to be proactive. The key is assessing your risk now and, if necessary, taking action to protect yourself. Here’s your seven-step plan for avoiding a widowmaker.
Getty Images
How to Prevent a Widowmaker Heart Attack
1. Understand your archenemy
A heart attack is caused by a blockage in an artery due to atherosclerosis, the process by which fatty deposits called plaque build up inside your pipes. But having crud in your arteries doesn’t necessarily mean you’re at imminent risk of a sudden, fatal heart attack. “The heart can tolerate a 40 or 50 percent blockage,” says Helene Glassberg, M.D., associate professor of clinical cardiovascular medicine at the University of Pennsylvania’s Perelman School of Medicine. “It’s like a pipe in your sink. If it’s half-clogged, you can still brush your teeth.”
You might start feeling chest pain with an artery blockage of about 70 percent or more. But blockages between 40 and 90 percent can cause a life-threatening heart attack. Underlying the vast majority of heart attacks is a problem akin to a zit popping, says Dr. Bailey. Plaque often forms as a soft, unstable deposit rather than a hard, stable one. (About 25 percent of heart attacks result from slow, gradual accumulation, which tends to produce calcified plaque.) A thin, fibrous cap on the plaque ruptures, and fatty material gushes into the bloodstream. Your body interprets this as an injury and releases clotting factors and platelets to seal the “wound.” Within minutes, a blood clot can form. Suddenly, a tolerable 40 or 50 percent blockage becomes a major obstruction. Cue the sirens.
Cells inside both types of plaque are inflammatory—meaning they attract ongoing immune-system attention—but soft plaque is more so. “Risk factors like smoking, eating processed foods, being overweight, and having high cholesterol make these cells angrier and more prone to rupture,” explains Dr. Glassberg. And therein lies an opportunity: By addressing these aggravating factors, you can reduce your risk of plaque forming and stabilize whatever amount you already have.
What’s New: Research finds that not all soft plaques rupture—and many rupture without causing a heart attack. So what distinguishes those that become potential killers? Investigators are working to figure out telltale danger signs in factors like plaque structure, development, and biology—even its temperature or acidity—using advanced technologies such as intravascular ultrasound and optical coherence tomography. No conclusions so far, but as imaging and computer modeling improve, researchers hope to refine their understanding of who’s at greatest risk.

Getty Images
2. Calculate your own heart attack risk
Plug “ASCVD” into a web browser and click on the American College of Cardiology’s ASCVD Risk Estimator Plus. Enter numbers for age, cholesterol (HDL and LDL), and blood pressure, and answer several yes/no questions. It’ll spit out a percentage that estimates your risk of developing atherosclerosis in the next 10 years. If you score 7.5 percent or higher, talk to your doctor about how to lower your risk. Don’t get hung up on whether any one number hits “normal” targets, which many cardiologists view as outmoded thinking.
“I’d rather talk about overall risk,” says Martha Gulati, M.D., cardiology chief at the University of Arizona College of Medicine–Phoenix. “It’s not just about one component.”
What’s New: According to a report from the Centers for Disease Control and Prevention, about one-third of adult men have not had a lipid profile in the past five years. Don’t be among them. To calculate your risk, you need to know your numbers, which is why it’s critical to have blood work done every four to six years starting at age 35.

Getty Images
3. Ask about these other important tests:
A coronary-artery calcium scan is a noninvasive test that looks inside coronary arteries to find actual plaque. It’s the best way to get a handle on your overall plaque risk, or “plaque burden.” Such scans may detect only firm, older, stable plaque, however, so they won’t necessarily predict an imminent heart attack.
“But if you have a lot of calcium, you probably have soft plaque as well,” says Dr. Glassberg. “Where there’s smoke, there’s fire.”
So establishing the presence of disease in this way can help guide treatment if other factors leave your doctor uncertain about your risk. More doctors are ordering a test for high-sensitivity C-reactive protein (hsCRP), a blood-component indicator of inflammation, higher levels of which are linked to heart-attack and stroke risk. (If you already know your hsCRP, go to reynoldsriskscore.org and fill out the Reynolds risk estimator, which determines your risk of cardiovascular disease in the next 10 years.)
What’s New: Too many patients who undergo invasive cardiac testing (e.g., coronary angiograms, catheterizations) don’t need it because no significant arterial obstructions are found. A new technology called HeartFlow (see sidebar, next page) is eliminating such guesswork and helping reduce health-care costs and improve patient experience. Using the data gathered from a noninvasive CT scan, HeartFlow creates a color-coded 3-D model of your coronary arteries and calculates how much any blockages are limiting blood flow. This allows cardiologists to more accurately assess who needs to go to the cath lab or undergo other treatments.

Getty Images
4. Factor in Uncle Fred:
Risk calculation isn’t foolproof. A recent study in the Journal of the American College of Cardiology found that half of the people without any cardiovascular risk factors still had at least early-stage atherosclerosis. “There’s a lot we don’t know about the genetics of heart disease,” says Dr. Glassberg. So it’s smart to consider your family history.
“If anyone in your immediate family had a heart attack, needed a stent, or had a diagnosis of atherosclerosis before age 55 for men and 65 for women, let your doctor know,” says Dr. Glassberg.
What’s New: A family history of heart disease could double your risk of having the condition yourself. So clueing your doctor in about family heart-disease experiences could influence the decision to start preemptive treatment with a risk-lowering medication like a statin, a Mayo Clinic study finds. People at intermediate risk who weren’t on meds but started them after understanding their genetic profile ended up with lower LDL (bad) cholesterol levels six months later in another Mayo Clinic study.

Shutterstock
5. Adopt a no-fad diet:
Each year brings another round of fad diets: lately raw, ketogenic, alkaline, Dukan, and Whole30. The worst thing you can do for your heart (and your overall health) is sample one after another as if they were tapas at a never-ending Spanish wedding.
Save yourself the effort and frustration. Diets don’t work because they’re not sustainable. Instead, remember this: An analysis of three major population studies linked eating high-quality, healthy foods to a lower risk of coronary-artery disease compared with eating low-quality, unhealthy foods, and that was independent of other risks like being inactive, overweight, or a smoker. So you don’t need to agonize over particular nutrients or even count calories as long as you’re consuming mainly foods like vegetables, fruits, whole grains, nuts, legumes, and yogurt, and relatively few foods like red and processed meats, refined grains, sweets, butter, and fried stuff.
What’s New: The DASH eating plan, which emphasizes the list of healthy foods mentioned above, was shown to be more effective at lowering blood pressure than any one antihypertensive drug, Dr. Gulati says.

Getty Images
6. Exercise the right way:
“I see men at the gym lifting heavy weights yet bulging with belly fat,” notes Steven Nissen, M.D., chair of cardiovascular medicine at Cleveland Clinic. “They may think they’re fit because they’re strong, but they’re not. You need to be aerobically fit.” Balancing strength and cardio is ideal, but resistance training generally won’t elevate your heart rate for extended periods the way a cardio workout does. Aim for the CDC-recommended 150 minutes of moderate-intensity (or 75 minutes of vigorous-intensity) cardio every week. People who did even half that minimum (about 15 minutes of moderate activity per day) lowered their mortality risk and added an average of three years to their life expectancy compared with inactive people, according to a Taiwanese study.
What’s New: Past research has shown the cardioprotective benefits of high-intensity interval training (brief bursts of activity followed by short periods of low-intensity recovery or rest).
A recent Australian review confirmed that, compared with moderate-intensity continuous exercise, HIIT sessions were a safe and effective way to improve cardiorespiratory fitness—even among people with coronary-artery disease. After a warmup, try fast-pace running or cycling for four minutes followed by three minutes at a lower intensity for four rounds, three days per week. Researchers found the greatest improvements occurred when participants trained in this manner for 7 to 12 weeks.

BraunS/Getty Images
7. Take your meds, if recommended:
Your doc may want you to take a cholesterol-lowering statin if your risk looks serious, even if you haven’t been diagnosed with heart disease. “Statins have demonstrated heart-attack risk reductions of 25 to 33 percent in part by limiting deposits of unstable plaques,” says cardiologist Matthew Feinstein, M.D., assistant professor of medicine and preventive medicine at Northwestern University’s Feinberg School of Medicine. They reduce inflammation, too.
What’s New: If statins prove ineffective or can’t be tolerated due to side effects, new PCSK9 inhibitors (Praluent, Repatha) can further reduce LDL cholesterol and lower heart-attack risk, says Dr. Bailey. Self-injected every two to four weeks, they’re often prescribed in addition to a statin but can be used independently. Either way, your doc may also want you to pop a daily 81 mg aspirin if your risk profile is intermediate or high, or if your plaque burden is substantial.
Steps like these turned Mowery’s life around after his heart attack. He eats mostly vegetables, fruit, and lean meats like fish and chicken, and logs 10,000 daily steps on his Fitbit. He’s lost 40-plus pounds, and his risk numbers look good. “My first question to my cardiologist at home was ‘Am I going to get back to normal?’ ” he recalls. “Her answer was ‘If you listen to me, you’ll be better than you were.’ I grew up 35 minutes from Philly and took a Rocky Balboa approach: ‘I’m not going down. I’m going to beat this.’”
You can, too.

Getty Images
What Happens If a Widowmaker Goes Untreated?
Without treatment, the mother of all heart attacks usually proceeds this way.
Source: Read Full Article